
Introduction
You have seen the headlines. A 22-year-old college athlete collapses on the basketball court. A 30-year-old mother drops dead in her kitchen. A 19-year-old soldier dies during basic training. In almost every case, the autopsy reveals a shocking truth: the victim had a genetic heart condition they never knew existed.
These stories are not rare anomalies. They are the tragic outcome of a massive blind spot in modern medicine. For decades, young people have been told they are “too young” to worry about heart disease. But for an estimated 1 in 200 to 1 in 500 young adults, a silent genetic time bomb is ticking inside their chest.
Unlike the lifestyle-related heart attacks we discussed earlier, genetic heart conditions often strike without warning. They do not give you chest pain for months. They do not show up on a routine physical. They can kill in an instant—unless you know to look for them.
In this article, we will uncover eight common genetic heart conditions that put young adults at risk. We will explain how they work. We will share real stories of those affected. And we will provide a clear roadmap for screening and prevention.
If you have a family history of sudden death, fainting, or heart problems, this article could save your life.
What Are Genetic Heart Conditions?
Genetic heart conditions are disorders passed down through families. They affect the structure or electrical system of the heart. They are caused by mutations in specific genes.
These mutations control how the heart forms, beats, or responds to stress.
Two Main Categories
1. Structural Cardiomyopathies
These are physical abnormalities of the heart muscle itself. The heart may become abnormally thick, dilated, or stiff. This leads to heart failure or dangerous arrhythmias.
2. Electrical Channelopathies
These are flaws in the ion channels that control the heart’s electrical impulses. The heart looks structurally normal. But its rhythm can suddenly degenerate into a deadly arrhythmia.
Why Are They So Dangerous?
The danger lies in their silence. Most young people with genetic heart conditions have no symptoms. They feel fine. Then a trigger occurs—intense exercise, extreme stress, or even a loud alarm. That trigger causes a fatal arrhythmia.
Many are discovered only after a family member dies suddenly. This is the cruel reality of genetic heart conditions.
How Genetic Heart Conditions Work
To understand why genetic heart conditions are so lethal, we need to look at two mechanisms.
Mechanism 1: Mechanical Failure
In cardiomyopathies, the heart muscle is weakened or abnormally structured. It may:
- Pump inefficiently, leading to heart failure
- Create areas of scar tissue, which act as electrical short-circuits
- Obstruct blood flow, especially during exercise
When blood flow is obstructed, fainting or cardiac arrest can occur. This is common in athletes with undiagnosed genetic heart conditions.
Mechanism 2: Electrical Chaos
In channelopathies, the heart’s electrical system is unstable. The sodium, potassium, and calcium channels misfire. These channels normally regulate each heartbeat.
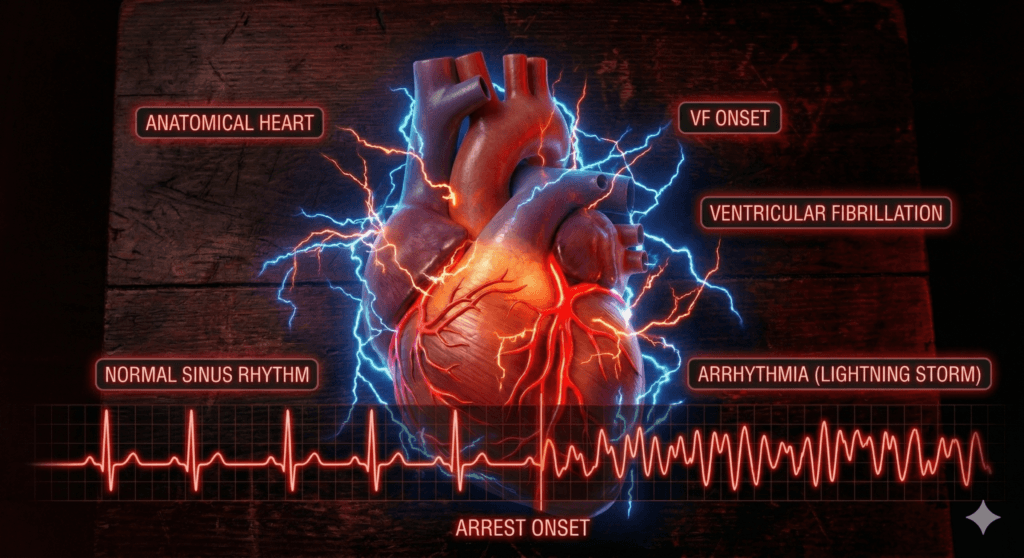
Under stress, this misfiring can trigger ventricular fibrillation. This is a chaotic rhythm where the heart quivers instead of pumping. Without immediate defibrillation, death follows within minutes.
Genetic heart conditions in this category are often invisible on standard tests.
The Exercise Connection
Many genetic heart conditions become symptomatic during physical activity. Exercise increases adrenaline. Adrenaline stresses both the heart muscle and its electrical system.
This is why athletes are disproportionately affected. They push their hearts to the limit. For someone with genetic heart conditions, that limit may be dangerously close.
Real-World Cases of Genetic Heart Conditions
These real stories show how genetic heart conditions can strike without warning.
Case Study 1: The High School Basketball Star
Profile: Male, 17 years old. Star athlete. No prior symptoms. Excellent physical condition.
The Event: During a game, he made a dunk. Then he collapsed. Teammates performed CPR. Paramedics arrived with an AED. He survived.
The Condition: Hypertrophic Cardiomyopathy (HCM) . This is the most common genetic heart condition. It affects 1 in 500 people. His heart muscle was abnormally thick. It blocked blood flow during exertion.
Case Study 2: The College Student Who Fainted
Profile: Female, 20 years old. She fainted once during a stressful exam. She fainted again while swimming.
The Event: After her second fainting episode, a cardiologist ordered an ECG. The test revealed a prolonged QT interval.
The Condition: Long QT Syndrome (LQTS) . This is a channelopathy. It can cause sudden fainting and cardiac arrest. She was started on beta-blockers. She was advised to avoid competitive swimming. Her genetic heart condition was now being managed.
Case Study 3: The Family Tragedy
Profile: A family with three siblings. The oldest brother died suddenly at 24 during a run. The family was devastated and had no answers.
The Event: The second brother underwent screening. He was diagnosed with Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) . The third sibling tested negative.
The Condition: ARVC replaces heart muscle with scar tissue and fat. It often affects the right ventricle. It is a common cause of sudden death in young athletes. This family learned that genetic heart conditions run in families.
Case Study 4: The Young Woman With Seizures
Profile: Female, 19 years old. She had been treated for epilepsy for two years. Her “seizures” occurred during exercise or emotional stress.
The Event: A new cardiologist ordered an ECG. The test showed a prolonged QT interval. Her “seizures” were actually cardiac events.
The Condition: Long QT Syndrome (LQTS) . She had been misdiagnosed. This is common with certain genetic heart conditions. Once correctly diagnosed, she received an implantable defibrillator.
Warning Signs of Genetic Heart Conditions
If you or a family member experience any of these, seek a cardiology evaluation immediately:
- Unexplained fainting (syncope) during or after exercise, stress, or startle
- Family history of sudden unexplained death before age 50
- Unexplained seizures (sometimes misdiagnosed, actually cardiac)
- Palpitations that are rapid, sustained, or associated with dizziness
- Heart failure symptoms (shortness of breath, swelling) in a young person
- Chest pain during exercise that goes away with rest
- Unexplained near-drowning (can occur with fainting in water)
These signs may point to underlying genetic heart conditions.
The 8 Silent Genetic Heart Conditions
Here are the eight most common genetic heart conditions that threaten young adults.
1. Hypertrophic Cardiomyopathy (HCM)
What it is: Thickening of the heart muscle, usually the left ventricle.
Prevalence: 1 in 500 people.
Risk: Most common cause of sudden cardiac death in young athletes.
Detection: Echocardiogram or cardiac MRI.
2. Long QT Syndrome (LQTS)
What it is: Electrical disorder affecting heart rhythm repolarization.
Prevalence: 1 in 2,000 to 1 in 5,000.
Risk: Sudden fainting, seizures, cardiac arrest triggered by exercise or stress.
Detection: ECG and genetic testing.
3. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
What it is: Heart muscle replaced by scar tissue and fat.
Prevalence: 1 in 2,000 to 1 in 5,000.
Risk: Ventricular arrhythmias, especially during exercise.
Detection: Cardiac MRI, ECG, genetic testing.
4. Brugada Syndrome
What it is: Electrical disorder affecting sodium channels.
Prevalence: 1 in 2,000 to 1 in 5,000 (higher in Asian populations).
Risk: Sudden cardiac arrest during sleep or rest, often triggered by fever.
Detection: ECG with drug challenge.
5. Dilated Cardiomyopathy (DCM)
What it is: Enlarged, weakened heart muscle.
Prevalence: 1 in 250 to 1 in 500.
Risk: Heart failure, arrhythmias, sudden death.
Detection: Echocardiogram, genetic testing.
6. Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT)
What it is: Electrical disorder triggered by adrenaline.
Prevalence: 1 in 10,000.
Risk: Fainting and cardiac arrest during exercise or emotional stress.
Detection: Exercise stress test (arrhythmia appears with exertion).
7. Laminopathy (LMNA-Related Cardiomyopathy)
What it is: Genetic mutation affecting nuclear envelope proteins.
Prevalence: Rare but aggressive.
Risk: Heart failure, life-threatening arrhythmias, early death.
Detection: Genetic testing, echocardiogram.
8. Short QT Syndrome (SQTS)
What it is: Electrical disorder with abnormally short QT interval.
Prevalence: Extremely rare.
Risk: Atrial and ventricular fibrillation, sudden death.
Detection: ECG showing short QT interval.
These eight genetic heart conditions account for the majority of sudden cardiac events in young people.
The Future of Genetic Heart Conditions Screening
The future of preventing sudden death lies in proactive screening. Genetic heart conditions are detectable. But only if we look for them.
The Athlete Screening Debate
There is ongoing debate about mandatory ECG screening for young athletes. Italy has implemented mandatory ECG screening for athletes. They have seen a 90% reduction in sudden cardiac death.
In the United States, screening remains voluntary. But awareness is growing. Many experts argue that screening for genetic heart conditions should be standard.
Cascade Screening
When a genetic heart condition is diagnosed in one family member, all first-degree relatives should be screened. This includes parents, siblings, and children.
This is called cascade screening. It can identify affected individuals before symptoms occur. It can save lives. Cascade screening is the most effective way to catch genetic heart conditions early.
The Role of Genetic Testing
Genetic testing can pinpoint the specific mutation in families with known conditions. It allows for:
- Risk stratification (knowing who is at highest risk)
- Lifestyle guidance (avoiding triggers like competitive sports)
- Family planning (options like preimplantation genetic diagnosis)
Genetic testing is transforming how we approach genetic heart conditions.
Implantable Defibrillators
For high-risk individuals with genetic heart conditions, implantable cardioverter-defibrillators (ICDs) can be life-saving. These devices detect and terminate dangerous arrhythmias. Modern ICDs are small and allow normal activity.
Expert Opinion on Genetic Heart Conditions
Dr. Barry Maron, MD, Director of the Hypertrophic Cardiomyopathy Center at Tufts Medical Center:
“Hypertrophic cardiomyopathy is the most common cause of sudden cardiac death in young athletes. The tragedy is that it is detectable with an echocardiogram. We need to move beyond the notion that young people are invincible and embrace screening for genetic heart conditions as a standard of care.”
Dr. Katherine W. Timothy, PhD, Genetic Counselor at the University of Utah:
“When a young person dies suddenly, families are often left with no answers. Cascade screening is essential. We can prevent the next tragedy by testing relatives. It is not just about the individual. It is about protecting an entire family line from genetic heart conditions.”
Dr. Christine Albert, MD, Chair of Cardiology at Cedars-Sinai:
“Genetic heart conditions are more common than most people realize. The challenge is identifying at-risk individuals before they have a cardiac event. Family history is critical, but it is not enough. We need broader screening.”
Expert Takeaways:
- ECG is not enough: For structural conditions like HCM, an echocardiogram is needed. For electrical conditions, an ECG is often sufficient.
- See a specialist: Not all cardiologists are trained in genetic heart conditions. Seek out a center specializing in inherited cardiovascular diseases.
- Don’t ignore fainting: Fainting in young people is often dismissed, but it can be the only warning sign of genetic heart conditions.
Recent Studies on Genetic Heart Conditions
Study 1: Prevalence of Genetic Heart Conditions in Young Athletes
Published in Circulation (2023)
Researchers screened over 1,500 high school athletes with ECG and echocardiogram.
- Key Finding: 1 in 200 athletes had a genetic heart condition that would have been missed by standard physical exam alone.
- Most common: HCM, LQTS, and ARVC.
- Conclusion: Current screening protocols miss many genetic heart conditions.
Study 2: Gender Differences in Sudden Cardiac Death
Published in JACC: Clinical Electrophysiology (2024)
Analyzed 20 years of data on sudden cardiac death in people aged 10–35.
- Key Finding: Males are 6 times more likely to die suddenly than females.
- But: Females are more likely to have missed warning signs (fainting) in the months prior.
- Conclusion: Better symptom recognition is needed for genetic heart conditions in young women.
Study 3: Cost-Effectiveness of Youth Screening
Published in JAMA Pediatrics (2023)
A cost-effectiveness analysis comparing universal ECG screening vs. standard pre-participation exams.
- Key Finding: Universal ECG screening was cost-effective when considering lives saved.
- Benefit was greatest in populations with higher rates of genetic heart conditions.
- Conclusion: Screening for genetic heart conditions makes economic sense.
Study 4: Genetic Testing in Sudden Death Victims
Published in New England Journal of Medicine (2024)
Researchers performed genetic testing on DNA from young sudden death victims.
- Key Finding: 40% had identifiable genetic mutations associated with genetic heart conditions.
- Most had no prior symptoms or known family history.
- Conclusion: Genetic heart conditions are significantly underdiagnosed.
Recent Research on Genetic Heart Conditions
1. Artificial Intelligence and ECG Interpretation
AI algorithms are being developed to detect subtle patterns in ECGs. Human eyes often miss these patterns. Early studies show AI-enhanced ECGs can identify genetic heart conditions with accuracy rivaling genetic testing.
This technology could make mass screening more feasible and accurate. AI could become a powerful tool for detecting genetic heart conditions early.
2. Gene Therapy and CRISPR
While still experimental, gene therapy for inherited heart conditions is advancing. Early trials for conditions like Danon disease (a rare cardiomyopathy) have shown promise.
CRISPR-based approaches are being explored to correct specific mutations in heart muscle cells. Gene therapy may one day cure certain genetic heart conditions.
3. Implantable Defibrillators in Young People
The use of subcutaneous implantable cardioverter-defibrillators (S-ICDs) is increasing in young patients with high-risk genetic heart conditions.
These devices can detect and terminate ventricular fibrillation. They do not require wires entering the heart. This reduces complications. Research is refining risk stratification to ensure the right patients receive devices.
4. Liquid Biopsy for Early Detection
Researchers are exploring “liquid biopsy” techniques. These analyze blood for genetic material released by damaged heart tissue. This could allow early detection of genetic heart conditions before symptoms appear.
5. Polygenic Risk Scores
New research combines multiple genetic variants into polygenic risk scores. These scores can identify individuals at higher risk for genetic heart conditions even without a single dominant mutation. This is an emerging frontier in prevention.
Conclusion
Genetic heart conditions are silent, stealthy, and potentially deadly. But they are not invisible. With awareness, proper screening, and proactive management, young people with these conditions can live long, full lives.
If you have a family history of sudden death, unexplained fainting, or heart disease at a young age, do not wait for symptoms. See a cardiologist. Get an ECG. Ask about genetic testing. Patients with these genetic conditions must avoid energy drinks.
If you are a young athlete, advocate for pre-participation screening that goes beyond a stethoscope. A simple ECG can detect many genetic heart conditions before tragedy strikes.
As we discussed in our article on heart attacks in youth, genetic factors are a critical piece of the puzzle. And as we explored in our article on stimulant dangers, energy drinks can be especially dangerous for those with undiagnosed genetic heart conditions.
Knowledge is the first line of defence. Your heart is precious. Protect it. Get screened for genetic heart conditions today.
FAQ: Genetic Heart Conditions:
Q1: If I have no family history, can I still have a genetic heart condition?
Yes. Approximately 30–40% of cases occur in individuals with no known family history. This can be due to a de novo (new) mutation. It can also be due to incomplete family information (small family size, adoptions, unknown paternity). Genetic heart conditions can appear without warning.
Q2: What tests should I ask for if I am concerned about genetic heart conditions?
ECG (electrocardiogram): Screens for electrical abnormalities.
Echocardiogram: Ultrasound of the heart to assess structure and function.
Exercise stress test: Can reveal arrhythmias or obstruction triggered by exertion.
Genetic testing: If a family mutation is known or if clinical findings suggest a specific condition.
Cardiac MRI: For detailed structural assessment.
Q3: Can I still exercise if I have a genetic heart condition?
It depends on the condition and its severity. Some conditions, like HCM, often require avoiding competitive sports. Others, like LQTS, may allow exercise with precautions. A cardiologist specializing in inherited conditions can provide a personalized exercise prescription. Never assume exercise is safe with undiagnosed genetic heart conditions.
Q4: How are genetic heart conditions treated?
Medications: Beta-blockers, antiarrhythmics
Lifestyle modifications: Avoiding triggers (certain drugs, intense exercise)
Implantable devices: ICDs for high-risk individuals
Procedures: Septal myectomy (surgery to remove thickened heart muscle) for obstructive HCM
Q5: Should my children be tested if I have a genetic heart condition?
Yes. Most genetic heart conditions are autosomal dominant. This means each child has a 50% chance of inheriting the condition. Screening should begin in childhood. Age-appropriate testing should be performed regularly. Early detection of genetic heart conditions saves lives.
Q6: What is the prognosis for someone diagnosed early with a genetic heart condition?
With proper diagnosis and management, most individuals with genetic heart conditions can live normal lifespans. The key is early detection. Avoid triggers. Adhere to treatment. Many people with genetic heart conditions live full, active lives with proper medical care.
Q7: Are there any warning signs I should watch for in my children?
Yes. If your child faints during exercise, gets unusually short of breath during sports, or has unexplained seizures, seek evaluation. Family history of sudden death under 50 is also a red flag. These could be signs of genetic heart conditions.
Q8: Can genetic heart conditions be cured?
Currently, most cannot be cured. But they can be effectively managed. Gene therapy research offers hope for future cures. For now, management focuses on preventing sudden death and managing symptoms.


")


